What Is Scoliosis?
Did you know that scoliosis, or abnormal lateral curvature of the spine, affects around 2-3% of the US population? That’s between six and nine million people! What’s more, according to the American Association of Neurological surgeons, approximately 38,000 people undergo spinal fusion surgery for scoliosis each year.
Since June is Scoliosis Awareness Month, let’s take some time to explore what the different types of scoliosis are, who they affect, and how they’re typically diagnosed and treated.
Scoliosis: definition and symptoms
When viewed from the side, the healthy spine has several curves in the sagittal plane. When viewed from the back, the healthy spine looks like a straight line from neck to tailbone.
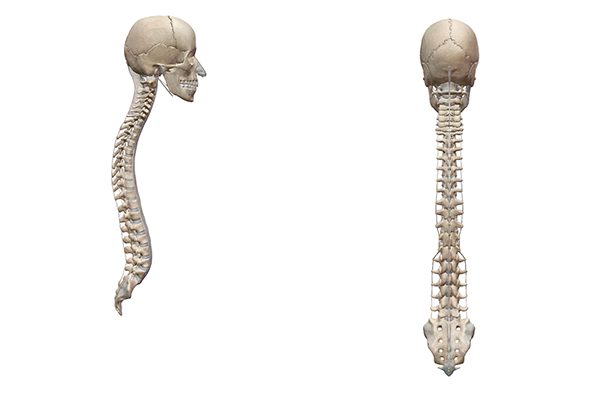
Lateral view of the spine (left) and anterior view of the spine (right) from Human Anatomy Atlas.
In scoliosis, however, the spine also has lateral (side-to-side) curvature, or curvature in the coronal plane. This gives the spine an “S” or “C” shape when viewed from the back, instead of a straight up and down appearance.
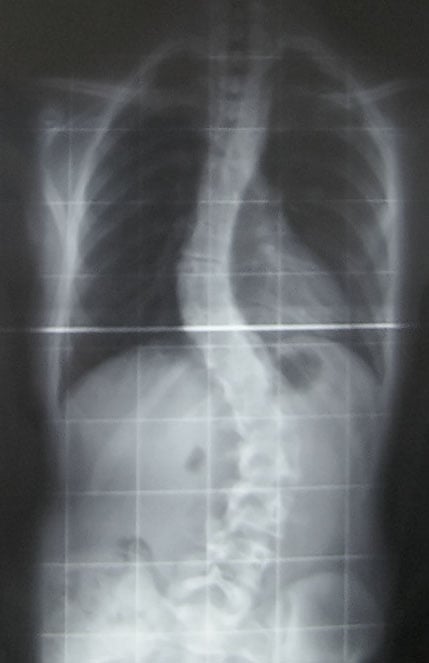 X-ray of the spine in idiopathic adolescent scoliosis. Image in the public domain, accessed via Wikimedia Commons.
X-ray of the spine in idiopathic adolescent scoliosis. Image in the public domain, accessed via Wikimedia Commons.
Diagnosing scoliosis usually involves a combination of a physical exam and imaging (X-Ray, spinal radiograph, MRI, or CT scan). In the physical exam, the AANS lists the following as common symptoms of scoliosis:
- Shoulders are uneven – one or both shoulder blades may stick out
- Head is not centered directly above the pelvis
- One or both hips are raised or unusually high
- Rib cages are at different heights
- Waist is uneven
- The appearance or texture of the skin overlying the spine changes (dimples, hairy patches, color abnormalities)
- The entire body leans to one side
Imaging is used to confirm the initial diagnosis and assess the severity of the curve(s): in general, less than 20 degrees is mild, 25-40 degrees is moderate, and 50+ degrees is severe. Depending on how severe the curve is, back pain or breathing problems may occur.
Most cases of scoliosis are diagnosed in childhood or adolescence (usually between the ages of 10 and 15). Many grade schools conduct scoliosis screenings for students that include the Adam’s Forward Bend Test, in which the patient stands with their feet together and then bends 90 degrees at the waist. This makes symptoms like the ones above easier for medical professionals to observe.
How is scoliosis treated?
Treatment for scoliosis varies based on the degree of curvature. For a mild curve, observation is usually the first course of action. If the curve progresses (that is, if it becomes more severe), then other treatment options will be considered.
Back braces, for example, are often used to help keep moderate curves in the spine from getting more severe as a child grows. There are several different types of braces—patients who need to wear a brace work closely with an orthopedic specialist to find one that will suit their individual needs. Proper use of a brace can sometimes prevent the need for surgery.
Still, surgery has proven to be an effective method of correcting severe curves and improving quality of life for adolescents with scoliosis. The most common type of surgery used to treat scoliosis is spinal fusion. In a spinal fusion procedure, the surgeon uses metal rods and screws to hold the curved section of the spine in place, correcting the curve, and uses small fragments of bone (a bone graft) to fuse several vertebrae together. Full recovery usually takes about a year.
Types of scoliosis
There are three main types of scoliosis—the classification is based on the etiology, or cause(s), of each one.
Idiopathic scoliosis
The most common type of scoliosis diagnosed in adolescents is idiopathic scoliosis. Idiopathic scoliosis accounts for around 80% of pediatric scoliosis diagnoses. “Idiopathic” means that there is no defined cause. However, people with a family history of idiopathic scoliosis often have an increased likelihood of developing it. Girls are more likely than boys to have progressing or severe curves—the exact reason for this is currently unknown. With early diagnosis and proper treatment, the outlook is good for people with idiopathic scoliosis. Normal function is often achieved, and pediatric idiopathic scoliosis patients go on to live active, healthy lives. That treatment can include observation, physical therapy, wearing a brace (for moderate cases), or surgery (for severe cases).
Congenital scoliosis
Congenital scoliosis is the least common type of scoliosis, occuring in 1 out of every 10,000 newborns. Because congenital scoliosis is a result of malformations to vertebrae that occur while a baby is still in the womb, it is present at birth. This means it typically gets diagnosed earlier than idiopathic scoliosis.
There are two main ways in which the spine can form atypically in congenital scoliosis. When a vertebra does not form completely, the result is a structure called a hemivertebrae. When vertebrae fail to successfully separate from one another during development, two or more vertebrae can be fused together by a bar of bone. Sometimes both types of abnormalities can occur in one case of congenital scoliosis.
Babies born with congenital scoliosis can have problems with other body systems and organs as well, specifically those systems that also develop around the same time as the spine (between 8 and 12 weeks of gestation). These can include the kidneys and bladder. Around 30% of congenital scoliosis patients also have issues with their spinal cord.
Doctors closely monitor the spinal curve(s) of babies and young children with congenital scoliosis and make decisions about treatment accordingly. Many children with congenital scoliosis undergo surgery. The type of surgical procedure—ranging from spinal fusion, to the removal of hemivertebrae, to the placement of “growing” rods or magnetic adjustable rods to correct a spinal curve—depends on a child’s individual case.
Neuromuscular scoliosis
Neuromuscular scoliosis is a type of scoliosis that is secondary to disorders of the nervous and/or muscular systems. It is often the result of conditions that impair the ability to control muscles that support the spine, such as cerebral palsy (CP) or muscular dystrophy. Spina bifida can also lead to neuromuscular scoliosis.
The most common treatment for neuromuscular scoliosis is spinal fusion surgery.
Scoliosis in children vs. adults
As mentioned above, scoliosis is usually diagnosed in childhood or adolescence. However, it is certainly not unheard of for idiopathic scoliosis to be diagnosed in an adult. Sometimes, what might have been a smaller curve during adolescence will progress further and become more severe. Adult idiopathic scoliosis occurs in the thoracic or lumbar spine, with similar symptoms to adolescent idiopathic scoliosis. Curves (and pain) may be worsened by the degeneration of the spine’s intervertebral discs.
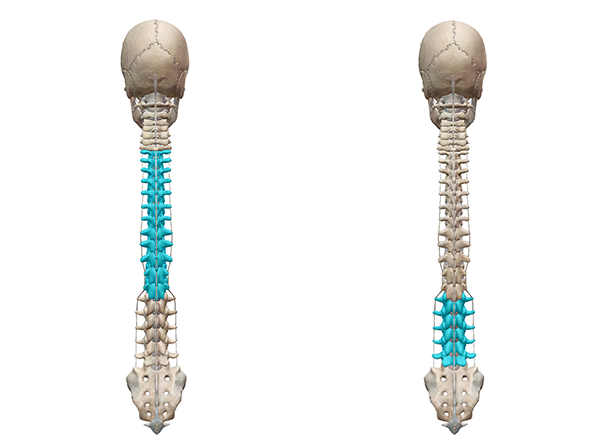
Thoracic spine (left) and lumbar spine (right). Images from Human Anatomy Atlas.
This leads us to a kind of de novo (new) scoliosis that is found in adults: degenerative scoliosis. Degenerative scoliosis is a result of disc degeneration, osteoarthritis in the joints between vertebrae, and/or the collapse of space between vertebrae. It typically occurs in the lumbar spine.
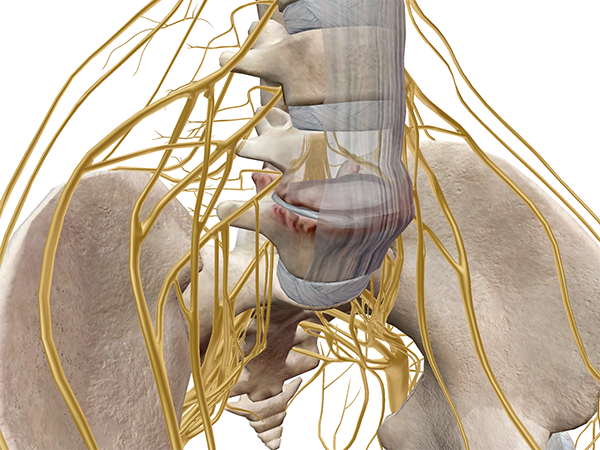 Collapsed intervertebral disc. Image from Muscles & Kinesiology.
Collapsed intervertebral disc. Image from Muscles & Kinesiology.
Common symptoms include numbness, back pain, and shooting pain that travels down to the legs.
Scoliosis treatment options are a little different for adults. Most cases of adult idiopathic scoliosis can be managed with nonsurgical treatments such as over the counter pain relievers, exercises, short-term brace use, and nerve blocks/epidural injections.
However, if pain is severe and a person’s quality of life is seriously reduced by their scoliosis, there are several different types of surgical procedures that can help restore function and relieve pain long term, including microdecompression (which relieves pressure on the nerves), surgical stabilization, fusion, osteotomy (spinal segments are cut and realigned), or vertebral column resection.
Although scoliosis can be painful and lead to further health complications if it is very severe, there is a wide range of treatment options available to both children and adults. To learn more about the Scoliosis Research Society’s National Scoliosis Awareness Month campaign, you can visit their website here. They have a great collection of resources for scoliosis patients of all ages, as well as family members and the general public.
June is also Aphasia Awareness Month and Alzheimer’s Awareness Month! Check out these VB Blog posts for more information:
Be sure to subscribe to the Visible Body Blog for more anatomy awesomeness!
Are you an instructor? We have award-winning 3D products and resources for your anatomy and physiology course! Learn more here.
Additional Resources


{kind=link}